Published by the Veer Care Editorial Team
Important Community & Patient Notice Based on a Real Case: The following article is developed directly from a real visual medical consultation between a subscriber and an actual licensed doctor on the Veer App. Not all medical consultations are adapted into clinical articles; we carefully select conversations addressing common, high-utility health questions to benefit our broader community.
Privacy & Anonymity Commitment: To protect patient confidentiality, all Personally Identifiable Information (PII) is strictly removed or sanitized before publishing. No names, exact locations, specific background histories, or identifying records are ever shared. For more details on our zero-sharing data guidelines, please read the Veer Care Privacy Policy.
The Query: “My 3.5-year-old has been crying inconsolably for 2 hours pointing to their ear. What should I do?”
During a late-night urgent care call on the Veer App, distressed parents connected with our pediatric specialist. Their 3-year, 6-month-old toddler had been crying continuously for over two hours, exhibiting extreme irritability, and repeatedly pointing toward their ear.
The parents asked:
What could be causing such sudden, intense ear pain without a fever?
How can we safely comfort the baby when they won’t even let us touch or examine the area?
What are the warning signs that mean we need to rush to an emergency room?
Here is the structured clinical guidance provided by the consulting Veer pediatric specialist.
1. The Dynamic of Toddler Ear Pain: Connecting the Past Illness
When a toddler experiences sudden, sharp ear pain, parents often look for an immediate external cause. However, pediatricians look at the child’s recent medical history. In this case, the parents noted that the toddler had recently been on cold and cough medication.
Even after the primary cold symptoms subside, a child’s unique anatomy sets them up for a secondary issue: Eustachian tube dysfunction.
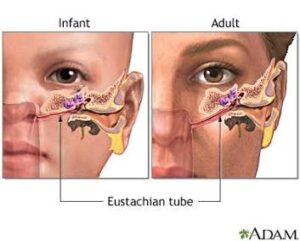
As shown in the medical reference diagram above, a toddler’s Eustachian tube (the canal connecting the middle ear to the back of the nose and throat) is shorter, wider, and significantly more horizontal than an adult’s. When a child has a cold, fluid can easily travel up this tube and become trapped behind the eardrum. As the child lies down to sleep, the shifting fluid builds up pressure against the delicate eardrum, causing a sudden, intense, throbbing pain—even if there is no active bacterial fever.
2. Virtual Triage Challenges: Navigating the Defensive Toddler
During the visual consultation, the Veer doctor guided the parents to look for two primary physical signs of localized infection:
Lymph Node Enlargement: Swelling in the lymph nodes directly beneath or behind the painful ear.
Throat Redness: Redness or swelling at the back of the mouth, which frequently co-occurs with middle ear inflammation.

However, because the toddler was in significant pain and highly irritable, they naturally refused to let their parents touch their ear or look inside their mouth.
Our pediatric panel emphasizes that this is entirely normal. Forcing a physical exam on an distressed, uncooperative child can heighten their anxiety, increase blood pressure, and actually worsen the throbbing pain in the head. In these high-friction situations, virtual doctors pivot directly to safe, empirical symptomatic relief rather than forcing physical manipulation.
3. The Immediate Pediatric Comfort Protocol
To relieve the pressure and ease the toddler’s distress, the Veer doctor prescribed a safe, temporary medical and physical routine:
Anti-Inflammatory & Pain Relief: The doctor advised a calculated dose of Paracetamol (Acetaminophen) based on the child’s exact weight. Paracetamol serves a dual purpose here: it safely blocks the pain signals and works as a mild anti-inflammatory to calm the irritated tissues around the eardrum.
Targeted Pediatric Decongestant: A specific pediatric decongestant was introduced. By reducing swelling in the nasal passages and the back of the throat, decongestants help open up that tiny, horizontal Eustachian tube, allowing the trapped fluid behind the ear to naturally drain away and relieve pressure.
Physical Thermal Comfort: The parents were instructed to keep the baby warm. Cold drafts can cause involuntary muscle contractions around the neck and jaw, which can intensify the perception of ear pain. A warm environment helps the surrounding muscles relax.
4. Red Flags: When to Transition to In-Person Emergency Care
Most fluid-pressure ear pains begin to subside within 30 to 45 minutes of administering pain medication and keeping the child upright. However, the doctor provided the parents with a strict checklist of Warning Signs. If any of the following occur, the child must be taken to an in-person clinic immediately:
Uncontrollable, High Fever: The sudden onset of a high fever that does not drop even after giving Paracetamol.
Ear Discharge: Any fluid, pus, or blood leaking out of the ear canal (a sign of a potential eardrum perforation).
Inconsolable Crying: Continued, agonizing crying that lasts longer than 1 to 2 hours after the proper dose of pain medication has been absorbed.
Physical Changes: Sudden swelling, severe redness, or protruding skin directly behind the outer ear flap (signs of a rare but serious infection called mastoiditis).
How to Get Instant Guidance for Your Child
Watching your child cry in pain is one of the most stressful experiences a parent can face. If your little one wakes up screaming, pulling at their ears, or showing signs of sudden distress, don’t face it alone in the dark. Open your Veer App and hit “Urgent Care” Within minutes, you’ll be face-to-face with an expert pediatrician who can assess your child virtually, guide your next steps calmly, and help you get your peace of mind back.